|
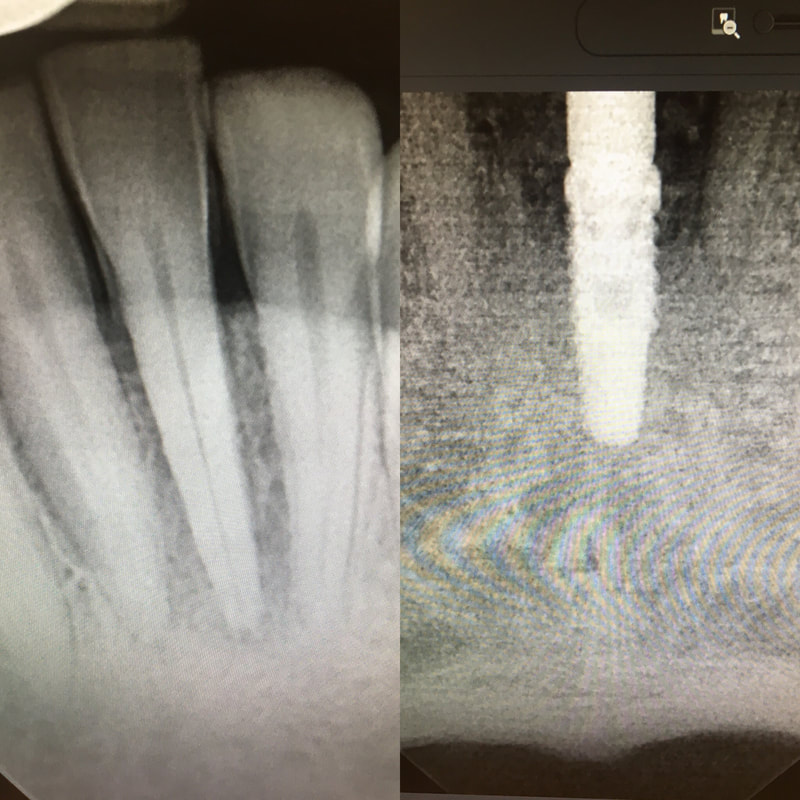
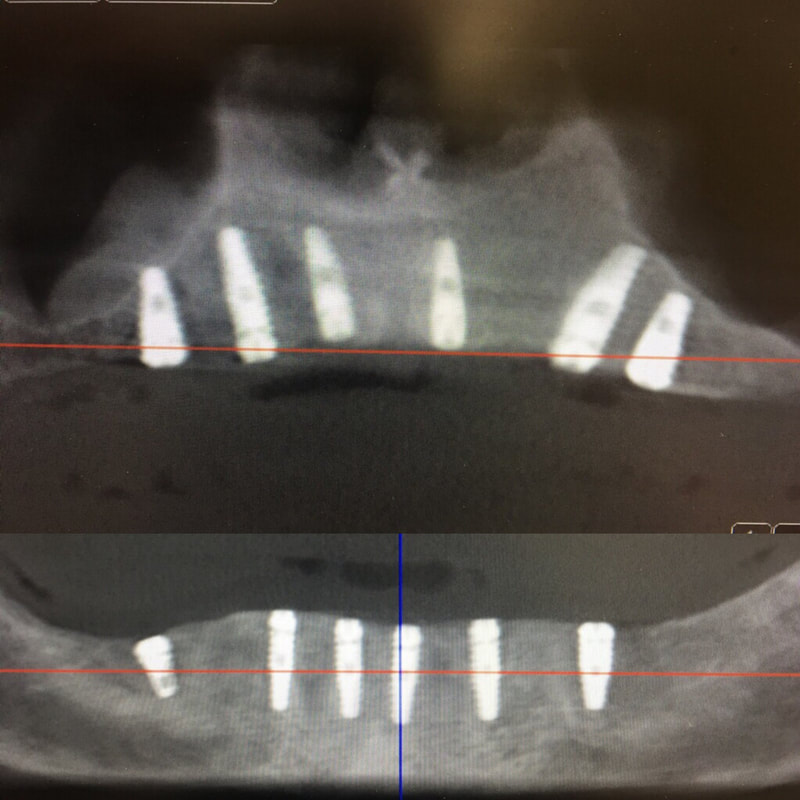
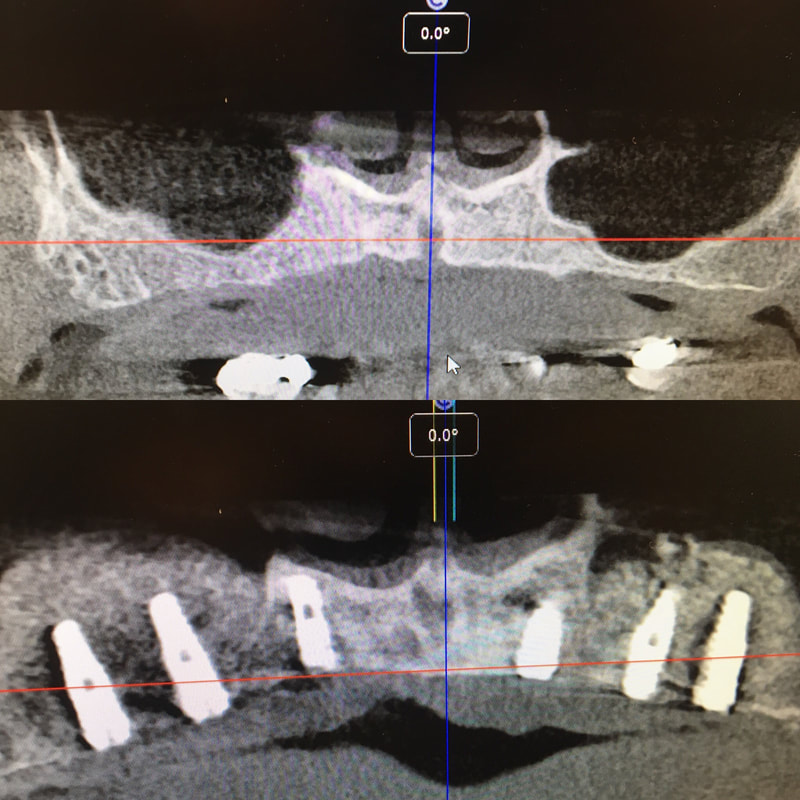
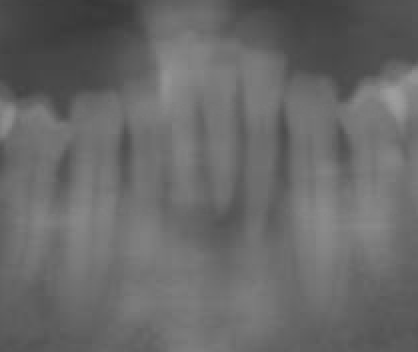
A few radiographs from my implant continuum. Starting with online and classroom sessions, progressing to model and pig jaw placement and culminating in live surgeries on those who need it the most - homeless veterans. The breadth of experience varied from single and doubles all the way to full mouth extraction with 6 upper and lower extractions and grafting. All implants will also be restored at no charge for the patients. All cases were treatment planned chair side with CBCT and placed freehand. I managed this 17 year old patient for the majority of her ortho treatment & was happy to finish the case. On the day her braces were removed, I used a custom matrix to create a lingual composite shell and then free hand sculpted the composite veneers on #7 & 10. The patient and her mother were happy with the result. One of my mentors on campus likes to say is good to know where you are going before you start, especially with complicated cases. This patient lost posterior teeth years ago and subsequent occlusal trauma caused her upper anteriors to flare forward horizontally and become mobile. She's already lost #8. Her treatment plan involves #7-10 implant bridge, ext #25, lower arch limited ortho, and posterior RPD. For this case, I digitally extracted #25 in Meshmixer and did a digital waxup for the ortho in Blue Sky Plan. Then I 3D printed the result on my Robox. Now that I have this model, I can mount it to oppose her existing upper teeth and determine a reasonable estimate for the position of her final #8-10 bridge. Digital workup, preemptively planning orthodontic movement is not the future but the present in dentistry today. I recently had the opportunity to purchase a used Cel-Robox printer. Last year I took a 3D Printing CE course with Rick Ferguson DDS. After calibrating the printer to Rick Ferguson's settings, I decided to practice my course knowledge with a sample case. I merged the .stl and .dicom files and then planned the implant and subsequent guide in Blue Sky Plan software for an ideal screw retained #19. While freehand implant placement is perfectly acceptable, being able to use computer guided precision to implants is a great tool for some cases.  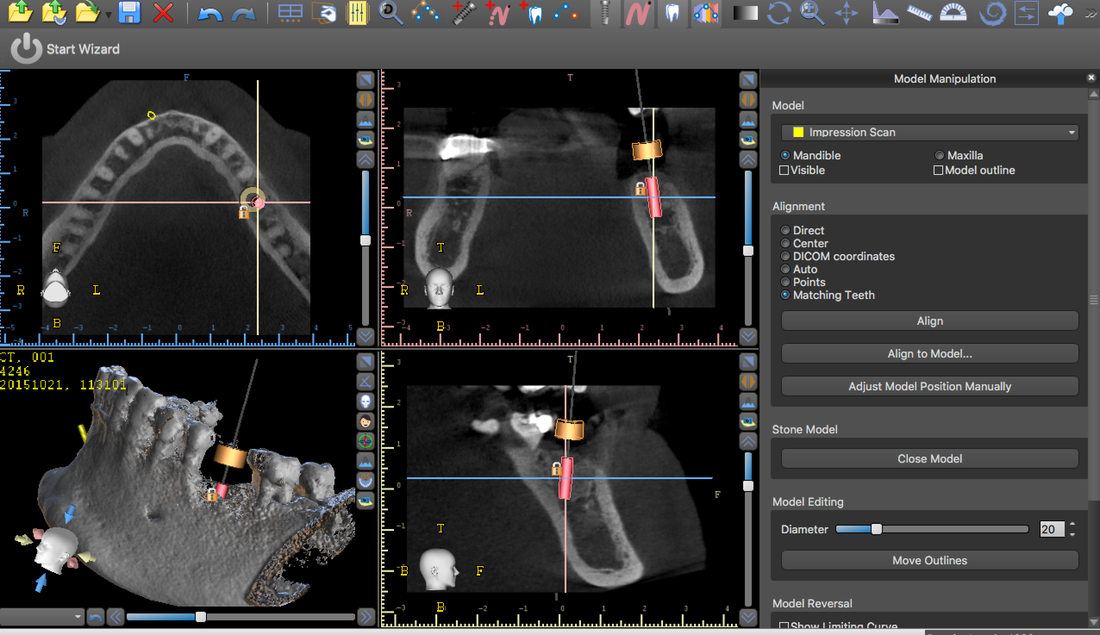 This patient fractured 2 PFM implant crowns and presented with a 6mm healing abutment before seeking treatment with me. His surgeon placed the #19 implant too distal, essentially causing a mesial cantilever within this molar. Rather than make him a third crown we decided to create a long lasting prototype he could wear for a few months to diagnose the occlusal interference causing the failures. I also reduced the buccal-lingual dimension to reduce occlusal forces and eliminate mesial contact entirely. Additionally, this prototype needed to re-create papilla as it had flattened after wearing the healing abutment for several months. Will be tracking patient monthly for 4 to 6 months and create new definitive restoration once comfortable the occlusion is successfully managed. Update Feb 2018 - this patient finally received his final crown; after a few months without incident, my prototype was removed from the implant was duplicated in pressed eMax and delivered to a happy patient. Here are before & after radiographs of some of the root canal treatments that I've completed. I have experience with rotary and hand instrumentation; cold lateral and warm vertical condensation; and comfortable using a microscope or loupes for all steps of the procedure. I took over this case 4 years after implants were placed. He came in due to broken healing abutment and decided to finally make prosthesis that utilized the implants Uncontrolled diabetic came in for tooth pain on lower front. Perio involved. class II mobility. Blood glucose tested 312 mg/dl. sent off for med consult and then extracted 23-26. delivered immediate resin rpd. Then hygiene and caries control. 3 months later diabetes is well controlled with daily average BG under 100 mg/dl. Preps, final impression and provisional fabricated in 1 appointment. FPD design: ovate pontics, 1mm metal margin for hygiene and beneath smile line so esthetically not an issue. Good outcome for a great patient who has a new lease on life with her oral & systemic health now under control. |